
Solution-How action potential of cardiac cells will be
Pharmacology of Arrhythmias
Case study-based activity. Patient with irregular cardiac rhythm
On winter morning, Dr. CA, a 56-year-old professor, is lecturing on the treatment of cardiomyopathies to the second year university students. He feels his heart beating irregular and becomes nauseated. He is able to finish his lecture but he continues to feel significantly short of breath throughout the morning. His persistent symptoms prompt him to walk down the street to the local emergency department.
Physical examination reveals an irregular heart beat ranging from 120 to 140 beats/min. Dr.CA’s blood pressure is stable (132/76 mmHg), and his oxygen saturation is 100% on room air. An electrocardiogram (ECG) confirms that Dr. CA has atrial fibrillation, without any evidence of ischemia. Several intravenous boluses of diltiazem are administered, and his heart rate decreases to a range of 80 – 100 beats/min but his rhythm remains irregular. Further laboratory studies and chest x-ray do not reveal an underlying cause for Dr. CA’s atrial fibrillation.
During observation over the next 12 hours, Dr. CA remains in atrial fibrillation. Although his heart rate is under better control, he continues to experience palpitations. Under continuous ECG monitoring, a cardiologist administers an intravenous injection of ibutilide. Twenty minutes later after receiving the ibutilide, Dr. CA’s ECG shows a return to normal sinus rhythm. Based on his age and generally good health, Dr. CA is sent home with a prescription for aspirin.
He is instructed to call his doctor if he develops further symptoms of atrial fibrillation.
Dr. CA. feels fine at first, but he develops recurrent palpitations within 3 weeks of his initial event. After discussion with cardiologist, he elects to start amiodarone at a maintenance dose of 200mg/day, in addition to continuing aspirin. Dr. CA. tolerates the amiodarone well and reports no difficulty breathing. He remains symptom-free during the rest of his cardiology lectures.
QUESTIONS:
1. Why did diltiazem slow Dr. CA’s heart rate without affecting his underlying heart rhythm, atrial fibrillation?
2. Why should ibutilidebe administered only under carefully monitored circumstances?
3. Why were ibutilideand amiodarone effective in converting Dr. CA’s rhythm to normal?
4. What adverse effects of amiodarone could develop at higher daily doses or during prolonged period of treatment (6 or 12 months)?
5. How action potential of cardiac cells will be affected by the antiarrhythmics given to him for the treatment?
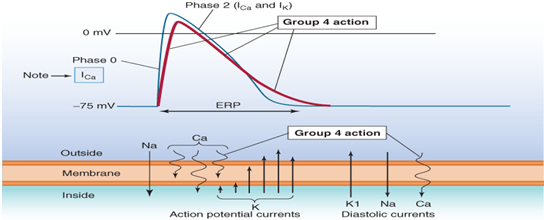
5 A. Diltiazam IV
5B. Ibutilide IV.
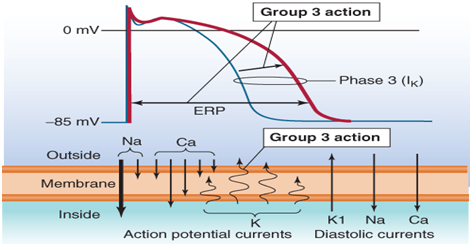
5. C. Amiodarone
6. Present the most common side effects and reasons for monitoring in case of use of these antiarrhythmics:
6A. Diltiazam IV
6B. Ibutilide IV
6C. Amiodarone IV –